Uploaded by
q
Aging and Photobiology of Vitamin D3

236
S-7-3
Aging
on the
Photobiology
M. F. HOLICK,
Vitamin
Boston
D,
City
of Vitamin
Z. Lu,
Bone and Skin Laboratory,
Hospital,
80 East Concord,
and
D3
T. C. CHEN
Boston
University
Boston,
MA
02118
School
of
Medicine
and
Introduction:
It
is
vitamin
D
photons
(that
energies
is
casual
exposure
are
not
between
absorbed
When
by
a
The
a
dermal
[1,
315
capillary
UV
Once
bed
its
it
ozone
layer
into
this
including
by
D3
transported
to
a
a
is
the
earth)
in
the
with
where
photolysis
for
its
of
7-
process
the
first
(7-
compound,
dependent
from
it
D3
labile
temperature
liver
their
energy
dermis
thermally
translocated
the
high
provitamin
results
D3,
system
and
with
the
envelopes
epidermis
radiation
vitamin
humans
sunlight,
that
the
Previtamin
triene
is
most
to
molecules
of
D3.
formed,
where
exposed
absorbing
absorption
of
D3.
thin
provides
is
penetrate
previtamin
rearrangement
vitamin
that
skin
the
nm
of
to
undergoes
form
by
and
variety
dehydrocholesterol
sunlight
human
absorbed
290
dehydrocholesterol).
to
to
requirement.
epidermis
to
hydroxylation
2].
Factors
that
Regulate
Recent
[4]
studies
profoundly
change
the
the
and
in
example,
in
number
the
year
[3]
During
promotes
(Fig.
both
age
D3
diminution
At
of
people
who
angle,
by
D3
November,
the
layer
were
previtamin
D.
mid-October
to
their
the
synthesis.
ozone
closer
in
winter
previtamin
by
to
D3
the
the
D3
of
between
lived
previtamin
day
to
oblique
previtamin
stratospheric
extended
of
due
absorbed
However,
the
was
this
photosynthesis
October.
time
is
during
efficiently
7-dehydrocholesterol
period
hand,
oblique
hours.
and
This
the
In
through
equator,
skin
in
Los
throughout
the
1).
summer
sunlight
Aging
of
[3]
D3.
more
are
penetrated
produced
in
cutaneous
ineffective
in
other
is
cutaneous
that
latitude
vitamin
afternoon
through
conversion
Rico,
the
the
to
the
which
the
the
D3
[3],
of
photons
March
this
season
late
in
(42•‹N),
(52•‹N),
Puerto
sun
and
photons
cause
On
and
the
resulting
315nm
Canada
exposure
of
from
Vitamin
synthesis
ultraviolet
layer
skin
mid-March.
provitamin
morning
Boston
to
Edmonton,
increasing
early
in
to
insufficient
changes
angle
of
that
cutaneous
zenith
human
290
Angeles
demonstrated
the
ozone
occurred
was
the
Synthesis
D3-producing
stratospheric
entire
have
solar
previtamin
For
Cutaneous
influence
in
months
the
before
in
producing
and
chronic
dermis
over
Boston,
exposure
production
10:00
concentration
Standard
D3
exposure
age
to
epidermis.
of
20
in
in
the
sunlight
from
D3.
Time
the
sunlight,
The
years
to
previtamin
Eastern
previtamin
and
the
of
sunrise
However,
(EST)
and
to
by
after
sunset
October,
15:00
EST
skin.
in
thickness
combination,
of
[5].
Simultaneous
epidermis
decreases
skin
causes
decreases
with
with
marked
linearly
these
increasing
with
changes,
the
age
[6].
M. F. HOLICK
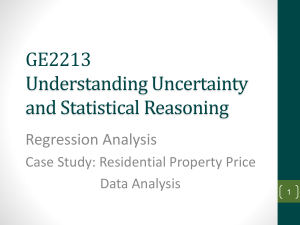
Figure
1, {3ƒ¿-3H}7-DHC
and
latitudes.
7-DHC
to
total
and
The
the
data
D3
to
Figure
volunteers
a
previtamin
sunlight
accurate
exposed
for
than
1
to•}1%
for
the
yr
12
calendar
results
the
January
in
except
Los
year
after
Angeles
for
h gave
the
Also
shown
exposure
(LA)
and
3
after
3h
the
May
months
same
to
photosynthesis
1
h
of
Rico
concentrations
of vitamin
radiation.
D in healthy
young
and
the
of
1986(•œ)(I),
of
7-
sunlight
(PR;
photoproduct).
to ultraviolet
in
1987,
where
within
same
result
in
is the
conversion
Puerto
and
(•¡-•¡)
to
For
the
of
h(•œ-•œ),
1986
months.
seasons
conversion
and
through
were
different
percent
(0-0)
1985
3
at
in
tachysterol)
the
for
1 and
1987
(0).
sunlight
1 h
and
measurement,
throughout
in
to
change
November
data
237
exposed
exposure
from
point
al.
annual
lumisterol,
when
exposure
is available
for
and
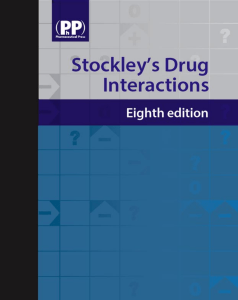
Circulating
D3,
more
D3
(•¢-•¢)
2.
after
compiled
single
was
(n=3)
collected
for
D3 in May
a 1 h value
Edmonton
samples
were
shows
of
previtamin
and
only
DHC
data
available
uncertainty
methanol
the•}2SD
(previtamin
figure
was
are
previtamin
photoproducts
Boston.
in
Shown
et
elderly
in
single
Symposium (7),
238
Aging
This is also reflected in the capacity of the elderly to produce vitamin D3 in their
skin. When healthy young and elderly subjects were exposed to simulated sunlight,
it was found that the amount of vitamin D in elderly subject's circulation over the
ensuing 72 hours was about 30% of healthy young volunteers [7](Fig. 2).
With the increased awareness of skin cancer due to chronic exposure to
sunlight, it has been recommended that before going outdoors people should always
apply a sunscreen.
The radiation that is responsible for causing skin cancer and
skin wrinkles is also the same radiation that is responsible for producing previtamin
D3 in human skin. As a result, the topical use of a sunscreen with a sun protection
factor of only 8 can prevent the cutaneous production of previtamin D3[8, 9].
Conclusion:
It is casual exposure to sunlight that provides most humans with their
vitamin D requirement.
The fortification
of milk in the United States has
eliminated vitamin D-deficiency
bone disease in children.
However, since the
elderly often suffer from a lactase deficiency and consider milk an unnecessary part
of their diet, they are at risk for developing vitamin D-deficiency and the resulting
bone disease osteomalacia [2, 10]. Indeed, there is mounting evidence in the United
States and in Europe that vitamin D-deficiency and osteomalacia are associated with
increased risk of hip fracture [10-14]. Vitamin D-deficiency in the elderly results in
secondary hyperparathyroidism.
This will exacerbate their osteoporosis as well as
cause a mineralization
defect in their bones resulting
in adult rickets or
osteomalacia.
The net effect of this process on bone is likely to weaken the bones
and increase their risk of fracture.
A recent epidemiologic survey in a controlled
nursing home environment
revealed that both free-living
and institutionalized
elderly who took a vitamin D supplement or drank 2 to 3 glasses of milk a day, were
vitamin D sufficient.
However, of those elderly who did not get a supplement of
vitamin D or drink milk, approximately 80% were borderline to overtly vitamin Ddeficient by the end of the winter [15]. Thus, it is recommended for the elderly,
that minimum exposure to sunlight in the morning or late afternoon in the spring,
summer and fall in the Boston area will provide them with their vitamin D
requirement and permit them to store any excess vitamin D in their fat for
utilization during winter months. People who live near the equator and are sensitive
to sunlight require less exposure. There is no need for the elderly to be exposed to
prolonged periods of sunlight since they can not increase their production of
previtamin D3. In Boston, it is during the first 15 to 30 minutes of exposure to
suberythemal doses of sunlight that is most beneficial, after this time they should
apply a sunscreen with a sun protection factor of at least 8 which will protect them
from the chronic damaging effects of excessive exposure to sunlight.
References:
[1]
Holick, M. F. (1989): Vitamin D: Biosynthesis, metabolism, and mode of action.,
DeGroot, L. J., Grune and Stratton, New York, pp.902-926.
[2]
Holick, M. F. (1990): Vitamin D and the skin: Photobiology, physiology and
therapeutic effecacy for psoriasis., ed. by Heersche, J., and Kanis, J., Elsevier
Science, Netherlands, pp.313-366.
M. F. HOLICK
et
al.
239
[3]
Webb, A. R., Kline, L., and Holick, M. F. (1988): Influence of season and
latitude on the cutaneous synthesis of vitamin D3: Exposure to winter
sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in
human skin. J. Clin. Endocrinol. Metab., 67, 373-378.
[4]
Holick, M. F., and Chen, T.: Vitamin D and skin function., in Pharmacology
Skin, ed. by Mukhtar H., Florida, CRC Press (in press).
[5]
Tan, C. Y., Strathum, B., Marks, R., et al. (1982): Skin thickness measurement
by pulsed ultrasound: Its reproducibility,
validation and variability. Br. J.
Dermatol., 106, 657-667.
[6]
MacLaughlin, J. A., and Holick, M. F. (1985): Aging decreases the capacity
human skin to produce vitamin D3. J. Clin. Invest. 76,1536-1538.
[7]
Holick, M. F., Matsuoka, L. Y., and Wortsman, J. (1989): Age, vitamin D, and
solar ultraviolet radiation. Lancet, November 4, 1104-1105.
[8]
Matsuoka, L. Y., Ide, L., Wortsman, J., MacLaughlin, J., and Holick, M. F.
(1987): Sunscreens suppress cutaneous vitamin D3 synthesis.
J. Clin,
Endocrinol. Metab., 64,1165-1168.
[9]
Matsuoka, L. Y., Wortsman, J., Hanifan, N., and Holick, M. F. (1988): Chronic
sunscreen use decreases circulating concentrations of 25-hydroxyvitamin
D.
Arch. Derm., 124, 1802-1804.
[10]
Holick, M. F., and Adams, J. S. (1990): Vitamin D metabolism and biological
function, in Metabolic Bone Disease, Avioli L.V. and Krane, S., eds. Orlando,
Grune and Straton, pp.155-195.
[11]
Holick, M. F. (1986): Vitamin D requirements
121-129.
[12]
Chalmers,
J.,
Osteomalacia--a
49B, 403-423.
[13]
Sokoloff, L. (1978): Occult osteomalacia in American patients with fracture
the hip. Am. J. Surg. Pathol., 2, 21-30.
[14]
Kavookjian,
H., Whitelaw, G., Lin, S., and Holick, M. F. (1990): Role of
vitamin D deficiency in the level of age-associated fracture in patients
treated at an inner city hospital. Orthopediac Trans., 14, 580.
[15]
Webb, A. R., Pilbeam, C., Hanafin, N., and Holick, M. F. (1990): One-year study
to evaluate the roles of exposure to sunlight and diet on the circulating
concentrations of 25-OH-D in an elderly nursing home population in Boston.
J. Clin. Nutr., 51, 1075-1081.
[16]
This work was supported in part by Grant #AR36963, #G06079 and Teaching
Nursing Home Grant #RR00533 from the National Institutes of Health.
for the elderly.
Conacher,
D. H., Gardner,
D. L.,
common disease in elderly women.
of
of
J. Clin. Nutr., 5,
and Scott, P. J. (1967):
J. Bone Joint Surg. (Br),
of