Turk J Med Sci
35 (2005) 175-177
© TÜB‹TAK
SHORT REPORT
Identification of a Novel Frameshift Mutation [Codon 3 (+T)] in a
Turkish Patient with β-Thalassemia Intermedia
Özlem GÜZELO⁄LU KAYIfiLI1, ‹brahim KESER1, Duran CANATAN2, Ahter fiANLIO⁄LU1,
1
1
Osman Nidai ÖZEfi , Güven LÜLEC‹
1
Department of Medical Biology and Genetics, Faculty of Medicine Akdeniz University, Antalya - Turkey
2
Antalya State Hospital, Thalassemia Center, Antalya - Turkey
Received: October 07, 2004
Key Words: β-thalassemia, β-globin gene, insertion, frameshift mutation, DNA sequencing
β-Thalassemia, one of the most widespread genetic
diseases in the world, is an autosomal recessive disease
generally caused by point mutations in the β-globin gene
that is located as a cluster on the short arm of
chromosome 11 (1-3). Modern molecular techniques
have provided a wealth of information about the nature
of mutations and their distributions within the world
population. More than 200 different mutations affecting
diverse levels of β-globin gene expression have so far
been identified (2,4,5). These mutations such as
frameshifts of the insertion/deletion type and/or
nucleotide substitutions have been reported to interfere
with the transcription of the β-globin gene, splicing
procedures and translation of β-globin mRNA (1-5). All
these mutations result in either an absence or reduction
of synthesis of β-globin chains (3,6). Insertion or deletion
of one or more nucleotides in the coding region of the βglobin gene disrupts the normal reading frame and causes
the frameshift. As a result of frameshift the β-globin
chain is synthesized as either elongated or truncated (7,
8).
We report a novel frameshift mutation in a 4-year-old
Turkish male with β-thalassemia intermedia. DNA
sequencing revealed a frameshift mutation with insertion
of thymidine at codon 3 (+T) and a G->A transition at
position 110 of intron 1. The co-inheritance of these
mutations (IVSI-110 and Cod 3(+T)) has not been
reported previously. For this reason, such cases may be
considered important in terms of understanding the
heterogeneity of molecular defects causing β-thalassemia.
A 4-year-old boy attended the Thalassemia Center in
Antalya State Hospital because of soft skin, anemia,
weakness, and lack of appetite. After clinical examination,
he was clinically diagnosed as having β-thalassemia
intermedia. He had received blood transfusions of 1 unit
annually. Hematologic data of the patient and his parents
are given in the Table. His blood counts were Hb; 9 g/dl,
MCV; 50.6 fl, MCH; 17.1 pg, and Reticulocytes; 2.63%.
HbA1, HbA2, and HbF levels were 64%, 3.7% and
32.4%, respectively.
DNA Analysis
DNA was extracted from whole blood using the
salting-out method (9). Polymerase chain reaction (PCR)
was performed using specific primers of the β-globin
gene and amplified DNA was analyzed to investigate
known common mutations in the Mediterranean region
using a β-globin strip assay kit (Vienna Lab) based on
reverse dot blot hybridization (RDBH), and a PCR-based
amplification refractory system (ARMS) as described
previously (10).
175
Identification of a Novel Frameshift Mutation [Codon 3 (+T)] in a Turkish Patient with β-Thalassemia Intermedia
Table. Hematological parameters of patient and his parents.
Patient
Mother
Father
Weight (kg)
11
60
80
Height (cm)
78
160
170
Liver (cm)
Normal
Normal
Normal
Spleen (cm)
Normal
Normal
Normal
Skin and mucosa
Normal
Normal
Normal
5.24
4.83
6.61
Hb (g/dl)
9
12.4
14.2
MCV (fl)
50.6
76.8
65.1
MCH (pg)
17.1
25.7
21.5
Reticulocytes (%)
2.63
-
-
HbA1 (%)
64
96
90,9
HbA2 (%)
3.7
3.7
6
HbF (%)
32.4
0.3
2.3
Ferritin
167.3
-
-
WBC x 109/l
12.3
5.1
5.6
Platelets x 109/l
417
256
195
RBCx1012/l
To explore the other mutations in the β-globin gene,
DNA including approximately 700 bp was amplified using
amplification primers (Primer F: 5’- GCCAAGGACAGGT
CGGCTGTCAT
C-3’
and
Primer
R:
5’CCCTTCCTATGACATGA ACTTAACCAT-3’) designed for
the initial site of the β-globin gene. PCR product was
separated in a 1.5% agarose gel. The amplified fragment
was isolated from agarose gel using purification kit (MBI
Fermantas, K0513). About 500 ng of purified fragment
was sequenced using the dideoxy termination procedure
of Sanger et al. (11). Before the samples were loaded on
sequencing gel, the gel was pre-run at 40 W. Then 4 µl
of each sample was loaded on denaturing 8%
polyacrylamide gel. After the gel had dried, it was
exposed to X-ray film for 12 h at room temperature and
then developed.
The G->A substitution at position 110 of intron 1 was
screened using RDBH and confirmed using ARMS. DNA
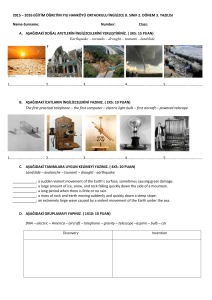
sequencing of the patient’s β-globin gene demonstrated
the insertion of thymine (+T) before the beginning of
codon 3 in exon 1 of the β-globin gene in the Figure. The
proband’s mother and father were heterozygote for
IVS.1.110 and codon 3 (+T), respectively. This mutation
disrupts the normal reading frame and causes the shift in
the protein reading frame.
176
Figure. Direct DNA sequence analysis of the mutated strand of a βglobin gene amplified fragment. The normal sequence is shown
on the left, and the abnormal allele (+T) on the right. The
inserted T at codon 3 is indicated by *.
The remarkable phenotypic diversity of β-thalassemia
in Turkey as well as worldwide reflects the heterogeneity
of mutations at the β-globin locus (12). More than 200
different mutations have been documented to date
(1,13), and more than 40 of these mutations have been
described by several Turkish laboratories for βthalassemia (12). We know that as these mutations affect
various levels of β-globin gene expression, they differ
greatly in their phenotypic effects. Despite this marked
molecular heterogeneity, the prevalent molecular defects
are limited in each risk population (12,13). Usually, 5 to
10 mutations account for the great majority of β-globin
disease-causing alleles in the at risk population. Mutation
analyses are available for common mutations and are
easily detected by PCR-based techniques. IVSI-110 was
the most common β-thalassemia defect with a frequency
of 38.6%, followed in decreasing order by IVSI-6
(9.4%), –30 (8.4%), IVSII-1 (6.9%), IVSII-745 (5.9%),
Cod44 (3%), and IVSI-1(3%), while frameshift
mutations were observed less frequentlyin our region
(14). Compound heterozygosity for mild/silent b+ and
Ö. GÜZELO⁄LU KAYIfiLI, ‹. KESER, D. CANATAN, A. fiANLIO⁄LU, O. N. ÖZEfi, G. LÜLEC‹
severe mutations produce a variable phenotype ranging
from β-thalassemia intermedia to β-thalassemia major
(1-3,6).
The frameshift mutation that occurred through
insertion of T at codon 3 can cause a truncated protein.
Therefore, when the +T is inserted as the 7th nucleotide,
Exon I ends at codon 6 with a stop codon (UGA) in mRNA.
The mild phenotype in our case may be due to the very
short truncated protein. Molecular analysis of βthalassemia has shown that many rare and several novel
β-globin mutations responsible for the disease are
present in the Turkish population, in addition to common
mutations.
with hemoglobinopathies in 1999. We believe that this
recording system is useful in controlling the disease and
in detecting many rare and novel mutations that are likely
to be important in our understanding of the
heterogeneity of molecular defects causing β-thalassemia
in our region.
Acknowledgment
This study was supported by the Akdeniz University
Research Foundation.
Corresponding author:
‹brahim KESER
Department of Medical Biology and Genetics,
Faculty of Medicine,
Akdeniz University,
TR-07070 Antalya - Turkey
E-mail: keser@akdeniz.edu.tr
The consanguinity rate in Antalya was reported to be
37% (15). Due to this relatively high rate, the high
incidence of β-thalassemia in the population and the
presence of rare and novel mutations in the rich genetic
pool in our region are not suprising. For this reason, our
group started to register all patients and their families
References
1.
Weatherall DJ, Clegg JB, Higgs DR et al. The hemoglobinopathies.
The Metabolic and Molecular Bases of Inherited Disease (Eds. CR
Scriver, A Beaudet, WS Sly, D Valle) McGraw-Hill, New York,
1989, pp: 3417-3483.
2.
Sack GH. Autosomal recessive disorders. Medical Genetics,
McGraw-Hill, New York, 1999, pp: 61-63.
3.
Oliveri NF. The beta-thalassemias. NEJM 341: 99-109, 1999.
4.
Trent RJ. Medical Genetics. Molecular Medicine, Longman
Singapore Ltd., Singapore, 1997, pp: 37-71.
5.
Ho PJ, Thein SL. Gene regulation and deregulation: a beta globin
perspective. Blood Rev 14(2): 78-93, 2000.
6.
Weatherall DJ. The thalassemias. The Molecular Basis of Blood
Diseases, 2nd Ed (Eds. G Stamatoyannopoulos, AW Nienhuis, PH
Majerus, H Varmus) WB Saunders, Philadelphia, 1994, pp: 157205.
7.
Enssle J, Kugler W, Hentze MW et al. Determination of mRNA
fate by different RNA polymerase II promoters. Proc Natl Acad Sci
USA, 1(90): 10091-10095,1993.
8.
Orkin SH, Goff SC. Nonsense and frameshift mutations in betathalassemia detected in cloned beta-globin gene. J Biol Chem 256:
9782-9784, 1981.
9.
Miller SA, Dykes DD, Polesky MF. A simple salting out procedure
for extracting DNA from human nucleated cells. Nucleic Acids Res
16: 1215, 1988.
10.
Newton CR, Graham A, Heptinstall LE et al. Analysis of any point
mutation in DNA. The amplification refractory mutation system
(ARMS). Nucleic Acids Res 17: 2305-2316, 1989.
11.
Sanger F, Coulson AR. A rapid method for determining sequences
in DNA by primed syntesis with DNA polymerase. J Mol Biol 94:
441-446, 1975.
12.
Tadmouri GO, Tuzmen S, Ozcelik H et al. Molecular and
population genetic analyses of beta-thalassemia in Turkey. Am J
Hematol 57: 215-20, 1998.
13.
Weatherall DJ. Phenotype-genotype relationships in monogenic
disease: lessons from the thalassaemias. Nat Rev Genet 2: 245255, 2001.
14.
Keser I, Sanlioglu AD, Manguoglu E et al. Molecular analysis of
beta thalassemia and sickle cell anemia in Antalya. Acta Haem
111: 205-210, 2004.
15.
Guz K, Dedeo¤lu N, Luleci G. The frequency and medical effect of
consanguineous marriages in Antalya, Turkey. Heriditas 111: 7983, 1989.
177